Osseodensification vs. Osseocompression
Two different ways to improve dental implant primary stability: bone-chip compaction with Versah Densah burs, and mechanical compression of trabecular bone through controlled undersized drilling. The clinical and biomechanical differences, and where the Crown Down 2-drill method fits in.

In implant dentistry, osseodensification has become well known because of the Versah Densah bur system and its associated clinical protocols. It is widely presented as a way to increase peri-osteotomy bone density and improve implant primary stability. [1-3]
However, another concept deserves more clinical attention: osseocompression.
Unlike osseodensification, osseocompression is not tied to a specific bur design or a single branded protocol. A degree of compression occurs during many implant placements as the implant threads and macrogeometry engage the osteotomy walls, creating mechanical pressure that contributes to primary stability. [4,5]
What is osseodensification?
Osseodensification is a drilling concept designed to compact bone particles rather than simply remove them, in contrast with conventional subtractive drilling, where every pass cuts bone away and evacuates it from the site. In the Densah bur protocol, burs are used in a counter-clockwise, non-cutting direction with copious irrigation, typically at 800 to 1,500 rpm. The goal is to push hydrated bone chips laterally and apically into the osteotomy walls. [1,3]
This can create a denser zone of compacted bone around the osteotomy, which may appear radiopaque on radiographs or CBCT imaging.
In simple terms, osseodensification attempts to use the patient’s own bone chips as autogenous grafting material instead of removing them from the site.
The main clinical goal is to increase peri-osteotomy bone volume and density to support primary stability and, in selected cases, assist with augmentation procedures. [1,2]

What is osseocompression?
Osseocompression is based on a controlled dimensional mismatch between the implant’s macrogeometry (taper, thread design, and thread depth) and the prepared osteotomy. During insertion, this mismatch generates mechanical compression of the surrounding trabecular bone, increasing implant-bone contact and contributing to primary stability.
When the osteotomy is slightly smaller than the implant diameter, the implant compresses the surrounding trabecular bone as it is inserted. [5,6] This increased mechanical contact between implant and bone can improve primary stability. [4,5]
The effect is most relevant in softer bone, where the trabecular structure has greater elastic compliance than cortical bone. The implant can condense the surrounding trabecular bone as it advances, creating a tighter mechanical fit. [7]
This is why undersized drilling is used by many implant systems to increase insertion torque and improve primary stability in low-density bone, including D3 and D4 bone in the Misch classification (soft cancellous bone with thin or absent cortical plate, common in the posterior maxilla). [5,6]
Clinical evidence of improved primary stability is most consistent in poor bone quality cases (D3 to D4 bone), where resonance frequency analysis often shows a higher implant stability quotient (ISQ) with undersized drilling compared to conventional sequences. [5,6]


How does osseodensification differ from osseocompression, side by side?
Same clinical goal (implant primary stability), different biomechanical pathway. Comparison values are drawn from published protocol documentation and peer-reviewed literature.
| Property | Osseodensification (Versah Densah) | Osseocompression (Crown Down) |
|---|---|---|
| Primary mechanism | Bone-chip compaction into osteotomy walls | Mechanical compression of trabecular bone |
| Required tooling | Specialized Densah burs (Versah) | Standard implant drills + undersized osteotomy |
| Drilling direction | Counter-clockwise (non-cutting) | Clockwise (conventional cutting) |
| Typical RPM | 800 to 1,500 rpm | Conventional implant-drilling speed |
| Irrigation | Copious external irrigation required | Standard irrigation; depends on protocol |
| Where it works best | Low-density (D3 to D4) bone, ridge expansion | Trabecular bone with sufficient elastic compliance |
| Limiting factor | Bur protocol + speed control | Cortical bone density (limits underdrilling) |
| Branded protocol? | Yes (Versah Densah) | No, technique-driven across implant systems |


Why do osseodensification and osseocompression share the same clinical goal?
Osseodensification and osseocompression share the same clinical endpoint: to improve implant primary stability. [4]
Osseodensification focuses on compacting bone particles into the osteotomy walls using specialized burs, high-speed reverse rotation, and abundant irrigation. One method is based mainly on bone-chip compaction. The other is based mainly on mechanical compression of trabecular bone.
Trabecular bone can generally tolerate more compression than cortical bone. Cortical bone behaves very differently: it is denser, less elastic, and less forgiving. If the osteotomy is undersized through the cortical plate, excessive insertion torque becomes a real risk. [5,7]
The surgeon may want to compress the trabecular bone to improve primary stability, but the cortical bone becomes the limiting factor. If the cortical portion is too tight, the implant may face excessive resistance before trabecular compression can be used safely or predictably. [5]
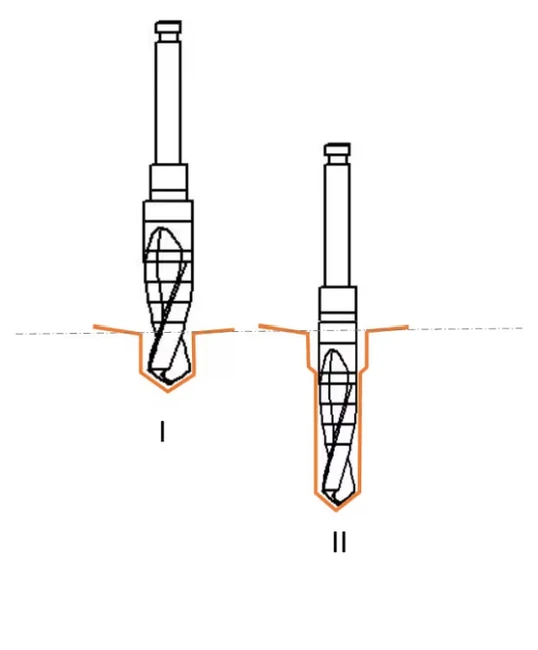
The Crown Down solution: separate the two zones
With the Crown Down 2-drill protocol, osteotomy preparation is performed with two tungsten carbide dental implant drills in two distinct stages:
- Stage 1 (cortical): the cortical bone is prepared according to the coronal requirements of the implant site, clearing the dense outer plate.
- Stage 2 (trabecular): the deeper trabecular portion is prepared with a smaller-diameter drill, allowing controlled undersized drilling. The cortical obstacle has already been addressed.
Once the cortical portion is properly cleared, the clinician can use the elastic potential of the trabecular bone far more effectively. The implant can condense the trabecular bone during insertion without being mechanically blocked by the dense cortical plate.
This makes osseocompression more controlled, more intentional, and more biologically logical.
Cortical-then-trabecular osteotomy
See the Crown Down difference
One kit, two drills per site, and a wear-proof carbide system designed to eliminate routine drill replacement.
Why this matters clinically
Primary stability is one of the most important factors in implant placement. It influences immediate loading decisions, healing confidence, and the clinician’s ability to predict the early mechanical behavior of the implant. [4]
Primary stability should not be achieved blindly. Too little stability is a problem. Too much uncontrolled compression is also a problem. [5]
The objective is not simply to generate the highest possible insertion torque. The objective is to create a stable implant environment while respecting the biological differences between cortical and trabecular bone and avoiding excessive compression.
Cortical bone and trabecular bone should not be treated as one single structure. They have different mechanical properties, they respond differently to drilling, and they respond differently to compression. They should be prepared with that difference in mind.
Standard one-size drilling protocols limit underdrilling because cortical bone cannot be compressed like trabecular bone. The Crown Down method addresses this problem by separating cortical preparation from trabecular preparation. That separation lets the clinician clear the cortical bone appropriately while preserving the ability to compress the trabecular bone for improved primary stability. For a deeper look at the underlying material and thermal science, see the clinical evidence behind Crown Down.
Conclusion
Osseodensification is mostly associated with Versah Densah burs and a specific drilling protocol that uses reverse rotation, abundant irrigation, and high speed, commonly 800 to 1,500 rpm in Densah bur protocols. [3]
Osseocompression results from the interaction between osteotomy preparation, implant macrogeometry, bone quality, and implant placement into a slightly undersized osteotomy, especially in the trabecular zone. [4,5]
The Crown Down drilling method makes it easier to control the degree of underdrilling by separating cortical and trabecular preparation. That separation allows the clinician to prepare the cortical bone properly, then use controlled undersized drilling in the trabecular bone to achieve better primary stability through intentional osseocompression. [5]
For a side-by-side look at how this protocol compares to other universal implant surgical systems, including Versah Densah, see the universal surgical kit comparison.
Frequently asked questions
Quick answers to questions clinicians ask most about this topic.
References
- 1. Padhye NM, Padhye AM, Bhatavadekar NB. Osseodensification: a systematic review and qualitative analysis of published literature. Journal of Oral Biology and Craniofacial Research. 2020;10(1):375–380. doi:10.1016/j.jobcr.2019.10.002.
- 2. Trisi P, Berardini M, Falco A, Vulpiani MP. New osseodensification implant site preparation method to increase bone density in low-density bone: in vivo evaluation in sheep. Implant Dentistry. 2016;25(1):24–31. doi:10.1097/ID.0000000000000358.
- 3. Huwais S, Meyer EG. A novel osseous densification approach in implant osteotomy preparation to increase biomechanical primary stability, bone mineral density, and bone-to-implant contact. The International Journal of Oral & Maxillofacial Implants. 2017;32(1):27–36. doi:10.11607/jomi.4817.
- 4. Javed F, Romanos GE. The role of primary stability for successful immediate loading of dental implants. A literature review. Journal of Dentistry. 2010;38(8):612–620. doi:10.1016/j.jdent.2010.05.013.
- 5. Orak B, Akgül M, Akdoğan T, Kahraman OE. Evaluation of implant primary stability using different drilling protocols: an in vitro study. BMC Oral Health. 2025;25:1306. doi:10.1186/s12903-025-06661-4.
- 6. Alghamdi H, Anand PS, Anil S. Undersized implant site preparation to enhance primary implant stability in poor bone density: a prospective clinical study. Journal of Oral and Maxillofacial Surgery. 2011;69(12):e506–e512. doi:10.1016/j.joms.2011.08.007.
- 7. Misch CE, Qu Z, Bidez MW. Mechanical properties of trabecular bone in the human mandible: implications for dental implant treatment planning and surgical placement. Journal of Oral and Maxillofacial Surgery. 1999;57(6):700–706. doi:10.1016/S0278-2391(99)90437-8.
Keep reading
Related reading
Explore related pages on the Crown Down dental implant drilling kit, protocol, and clinical science.
Protocol
The 2-Drill Implant Osteotomy Protocol
How drill #1 and drill #2 prepare the implant osteotomy in two steps.
Read moreBone Anatomy
Cortical vs. Trabecular Bone in Implant Surgery
Elasticity, rigidity, vascularization, and innervation of the two tissues — and why each requires its own drilling strategy.
Read moreProduct Catalog
Crown Down 2026 Catalog
Every kit, drill, SKU, and stopper in one printable PDF reference.
Read more